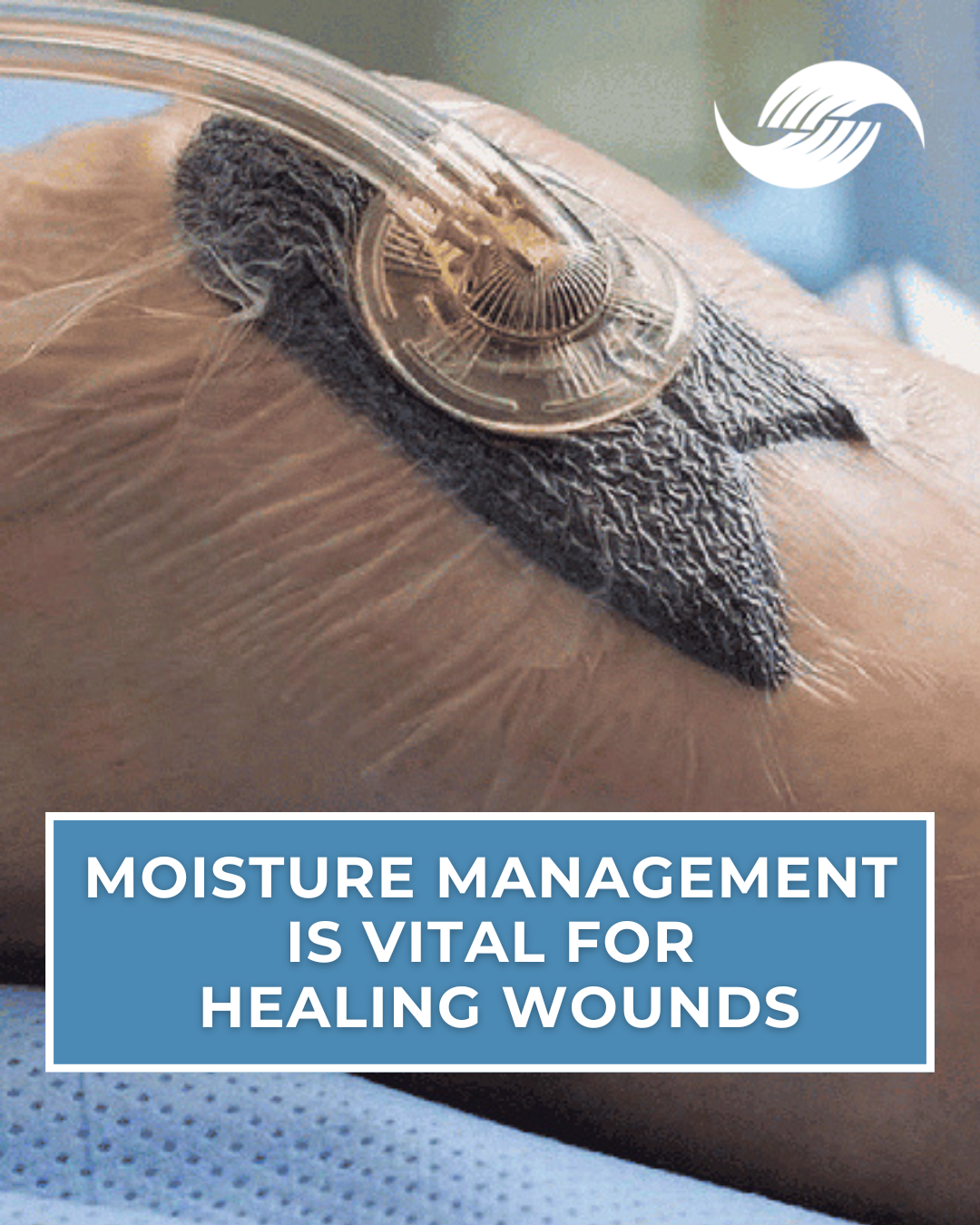
Calciphylaxis, a severe condition characterized by calcification of small to medium-sized blood vessels leading to skin necrosis and potential organ failure, and an incredibly high one year mortality rate of uo to 70%, has posed significant management challenges. Recent advances, however, have illuminated a promising treatment modality: vitamin K. Specifically, studies indicate that vitamin K's role in activating the matrix Gla protein (MGP) - an inhibitor of vascular calcification - addresses the core pathophysiology of calciphylaxis.
Traditionally, sodium thiosulphate (STS) has dominated as the primary treatment option, lauded for its calcium-chelating and antioxidant properties. However, its effects on patient survival remain questionable, with many studies showing no marked reduction in mortality. Additionally, adverse side effects like nausea, hypotension, and potential exacerbation of hypercalcemia further limit its applicability.
This brings us to the groundbreaking findings of a recent study. In the words of Dr. Sagar U. Nigwekar and colleagues:
"In a 12-week phase 2 study that enrolled 26 patients with calciphylaxis, Sagar U. Nigwekar, MD, MMSc, of Massachusetts General Hospital in Boston, and colleagues found that patients treated with oral phytonadione, a form of vitamin K, was associated with a significantly lower mortality rate compared with placebo at 12 weeks (0% vs 31%). In addition, phytonadione-treated patients experienced significant decreases in the size of a patient’s largest skin lesion, the combined size of all lesions, and pain intensity compared with placebo.” (1).
The implications of this study are profound. Not only does vitamin K supplementation show promise in reducing lesion size and pain intensity, but its potential to slash mortality rates to zero sets it apart from other treatment modalities like STS.
As the Chief Medical Officer of a Wound Care specialty group involved in treating Calciphylaxis in more than 100 facilities in the US, I am frequently called upon to direct treatment of patients with this condition. Since 2019, our group, based on evidence from the Mass General clinical trial referenced in this article, has been using vitamin K as a principal treatment strategy, with excellent results regarding wound healing and mortality risk. There have been no significant adverse events to date. What is discouraging is the fact that since 2019, our team has yet to encounter a clinician who is familiar with this treatment strategy.
We feel that vitamin K will supplant other treatment methods for Calciphylaxis for several reasons.
1. Targeted Action: Unlike STS, which offers a broader approach to symptom management, vitamin K directly rectifies the vitamin K deficiency that inactivates MGP, a crucial player in the pathophysiology of calciphylaxis.
2. Safety Profile: With an appropriately monitored regimen, vitamin K supplementation exhibits a favorable safety profile, overshadowing the numerous side effects associated with STS.
3. Mortality Reduction: The potential of vitamin K to drastically reduce mortality rates in calciphylaxis patients, as demonstrated in Dr. Nigwekar's study, is a breakthrough in itself.
What is also relevant is that vitamin K is found in two major forms: vitamin K1, or Phylloquinone, found mainly in green, leafy vegetables, and K2, or Menaquinone, found mainly in fermented foods that are uncommon in the US, such as Natto.
Importantly, vitamin K1 is mainly active in the liver, producing blood-clotting proteins. In contrast, vitamin K2 is primarily active outside the liver, which is responsible for activating Matrix GLA protein.
Vitamin K2 is 10 times as potent as vitamin K1 as an activator of Matrix GLA protein while being 1/10 as active in the liver in the synthesis of clotting factors, making it the better choice for the treatment of calciphylaxis because it activates that desired protein, while being less likely to foster a hyper-coagulable state.
In Dr. Nigwekar’s Mass General clinical trial, vitamin K1 was utilized (10mg PO, three times per week). Since most hospital formularies do not contain K2, we typically have utilized the vitamin K1 regimen for inpatients. Upon discharge, I believe it is preferable to transition the patient to vitamin K2, 1mg daily. There are a number of OTC vitamin K2 products, which contain from 90mcg to 1mg of K2.
We recommend choosing a preparation containing at least 600mcg of K2, which can be dosed as two capsules, PO daily. By transitioning to K2, therapy can become more specific in activating the desired Matrix GLA protein and limiting the risk of thrombotic complications. Studies such as Schurgers et al., 2007, have found no association between vitamin K2 intake and increased thrombosis risk (2).
While sodium thiosulphate served its purpose when options were limited, the dawn of a more effective treatment strategy is upon us. Vitamin K, by addressing the root cause of calciphylaxis, promises symptom relief and a profound reduction in mortality risk. It is incumbent on those involved in treating this disease to become familiar with vitamin K treatment for Calciphylaxis to reduce the morbidity and mortality risk of this condition.
1. Nigwekar SU, Krinsky S, Thadani RI, et al. Phase 2 trial of phytonadione in calciphylaxis. Presented at the American Society of Nephrology’s Kidney Week 2019 meeting held Nov. 5 to 10 in Washington, DC. Poster TH-PO1188.
2. Schurgers, L. J., & Vermeer, C. (2007). Determination of phylloquinone and menaquinones in food. Effect of food matrix on circulating vitamin K concentrations. Haemostasis, 30(6), 298-307